Restoring Study 329: efficacy and harms of paroxetine and
imipramine in treatment of major depression in adolescence
It's been eagerly anticipated, and everyone pretty much guessed what the conclusions would be, but it's finally official. The data from Study 329 show that paxil improved depression in adolescents no more than placebo (same for imipramine).
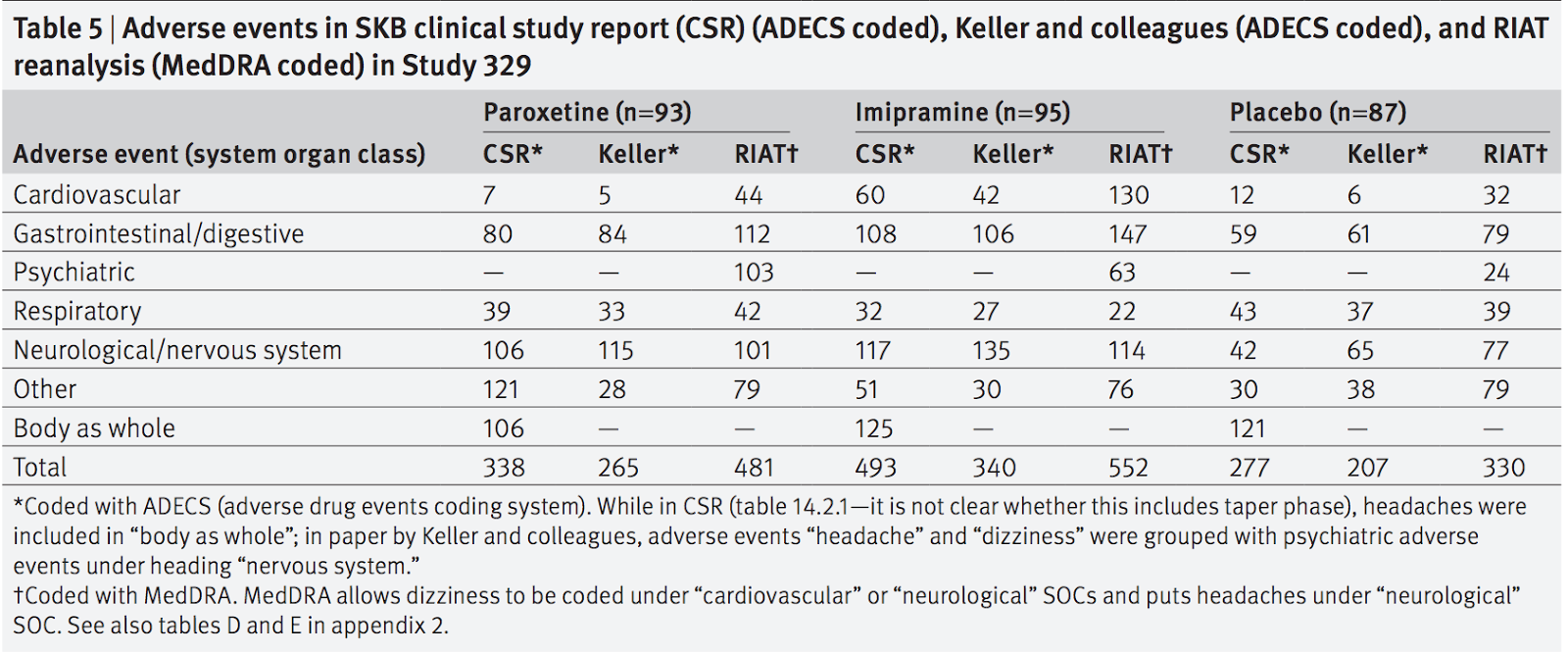
More importantly, from my perspective, since there are always some outliers who respond to meds others don't, are the adverse events. The re-analysis showed a lot more harm than the original. Paxil had a lot more psychiatric adverse events, such as suicidal behavior, and imipramine a lot more cardiovascular events.
Results
The efficacy of paroxetine and imipramine was not
statistically or clinically significantly different from
placebo for any prespecified primary or secondary
efficacy outcome. HAM-D scores decreased by 10.7
(least squares mean) (95% confidence interval 9.1 to
12.3), 9.0 (7.4 to 10.5), and 9.1 (7.5 to 10.7) points,
respectively, for the paroxetine, imipramine and
placebo groups (P=0.20). There were clinically
significant increases in harms, including suicidal
ideation and behaviour and other serious adverse
events in the paroxetine group and cardiovascular
problems in the imipramine group.
The reasons for the discrepancies are interesting. It seems like the difference in efficacy results was related to the fact that the original authors deviated from protocol, so that the same data give different results:
The marked difference between the efficacy outcomes as reported by us and those reported by SKB results from the fact that our analysis kept faith with the protocol’s methods and its designation of primary and secondary outcome variables.
The authors/sponsors departed from their study protocol in the CSR itself by performing pairwise comparisons of two of the three groups when the omnibus ANOVA showed no significance in either the continuous or dichotomous variables. They also reported four other variables as significant that had not been mentioned in the protocol or its amendments, without any acknowledgment that these measures were introduced post hoc. This contravened provision II of appendix B of the Study 329 protocol (“Administrative Matters”), according to which any change to the study protocol was required to be filed as an amendment/modification.
The difference in adverse events had to do with how the events were coded. The original article used a now obsolete and unavailable coding system, and the language in the Case Study Reports (CSR's) was often translated to something innocuous. I particularly liked one table which showed the ways that adverse events could be inaccurately reported:

As for GSK's reaction, the NY Times included this quote from the original authors:
Dr. Keller and his co-authors strongly disputed the reassessment of their work. In a joint statement, he and his team said they incorporated secondary measures before knowing which patients were taking Paxil and which were not — not afterward, as the new analysis claims, for some of the measures. “In summary, to describe our trial as ‘misreported’ is pejorative and wrong,” they conclude.
The authors of the new study, Joanna Le Noury, John M Nardo, David Healy, Jon Jureidini, Melissa Raven, Catalin Tufanaru, and Elia Abi-Jaoude, had their work cut out for them:
This RIAT exercise proved to be extremely demanding
of resources. We have logged over 250 000 words of
email correspondence among the team over two
years. The single screen remote desktop interface
(that we called the “periscope”) proved to be an enormous challenge. The efficacy analysis required that
multiple spreadsheet tables were open simultane-
ously, with much copying, pasting, and cross check-
ing, and the space was highly restrictive. Gaining
access to the case report forms required extensive correspondence with GSK.12 Although GSK ultimately
provided case report forms, they were even harder to
manage, given that we could see only one page at a
time. It required about a thousand hours to examine
only a third of the case report forms. Being unable to
print them was a considerable handicap. There were
no means to prepare packets for multiple independent coders, to decrease bias; to make annotations or
use margin comments; or to sort and collate the
adverse event reports. Our experience highlights that
hard copies as well as electronic copies are crucial for
an enterprise like this.
I think they deserve huge thanks.
So check out the study. And also check out Study329.org for the whole history, as well as multiple posts by authors Mickey Nardo at 1boringoldman.com and David Healy at Davidhealy.org and Rxisk.org.
I think they deserve huge thanks.
So check out the study. And also check out Study329.org for the whole history, as well as multiple posts by authors Mickey Nardo at 1boringoldman.com and David Healy at Davidhealy.org and Rxisk.org.