Collaborative Care is alive and scoring a 0 on the PHQ-9. The Clozaril REMS deadline was extended. Tom Insel left NIMH for Google. Mandatory E-prescribing was postponed until this coming March. EHRs continue to disappoint. Meds long past patent have had their prices jacked up 5000%. The FDA is looking to appoint a new head, and Robert Califf, a cardiologist with strong ties to the pharmaceutical industry has been nominated (See NY Times and David Healy).
On the upside, Dinah at Shrink Rap came up with a brilliant way for people to access psychiatric care in Maryland. I hope this approach is replicated more broadly.
I was perusing my posts from this past year, and I made a list of some of the major topics, and their respective posts, both general and personal:
Maintenance of Certification
I studied for:
The Montillation of MOC
Percentages
And passed:
Done
There and Back Again
Framed
Signed, Sealed, Delivered
Switching the Labels
my board recertification exam.
And I was certified by the NBPAS, as well:
Another Board

The ABPN refused to make any significant changes to MOC, especially Part IV:
I Really Should be Studying, But...
An MOC Step?
Follow the Money
Although the Part IV Feedback modules are now optional.
And I developed my own Psychoanalytic PIP Module:
Fascinating
Here Goes Nothin'
A Monkey's Uncle
The best part about all of this is that I've written enough MOC posts that I now misspell "Maintenance" only about 5% of the time.
Affordable Care Act (ACA)
The ACA has kicked in:
Out of Network Benefits in NY
And pushed me over the edge into the realm of blog ads:
Adding Ads and the ACA
Psychoanalysis
I terminated my analysis:
Termination
Blessings
And wrote some other posts about psychoanalytic evidence and topics:
Analytic Evidence
AA Brill
The Blank Screen
Narcissism, Part I
Narcissism, Part 2
Jeffrey Lieberman
His book, Shrinks was published:
"Shrinks" Review: Introduction
Shrinks: The Untold Story of Jeffrey Lieberman's Oedipal Victory over Papa Freud
Shrinks Links, Etc.
And a torrent of posts followed, culminating in the one about his fiasco of a presentation at the White Institute:
Lieberman Speaks
Addyi
The FDA approved a drug that could hurt you but can't help you:
They Caved
That was immediately sold for $1Billion:
Addyi-dendum
And then the FDA and Valeant pawned off responsibility onto the doctors who prescribe it, and the pharmacies that fill the prescriptions:
Addyi REMS-A Shanda
Paxil 329
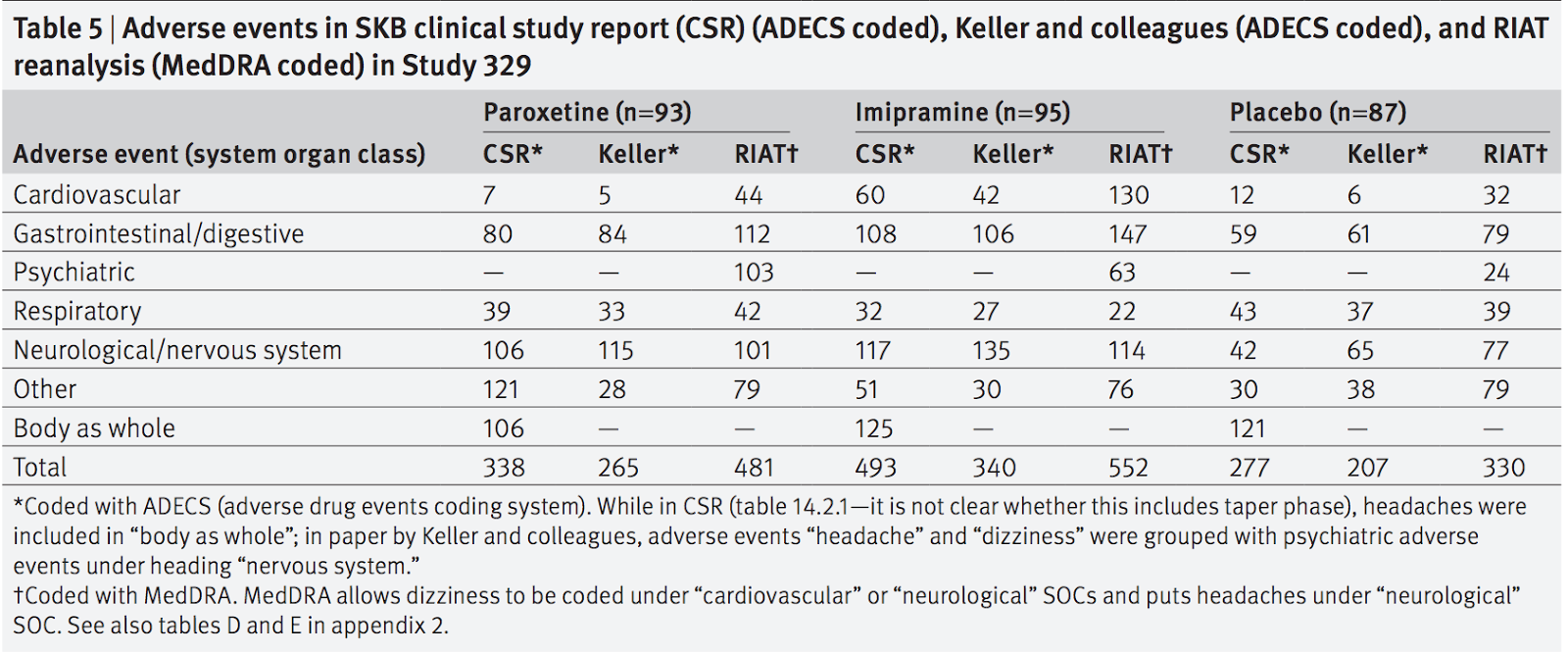
Finally, and perhaps most importantly, the restored version of Paxil Study 329 was published, with disturbing conclusions:
329
Do I have a favorite post from the year? Not really. The Lieberman posts, especially the reviews and the one about his talk at White took the most out of me. But in terms of content, I think the Analytic Evidence and 329 posts are the most important.
On to pastures greener.